
In the realm of neurodegenerative disease therapies, the conventional 'one disease–one target–one drug' approach has proven inefficient for multifactorial conditions like Alzheimer's disease (AD), Parkinson's disease (PD) or Amyotrophic Lateral Sclerosis (ALS). If you want to bring better therapies to patients, you must embrace a network-based mindset and consider pursuing multi-targeted drugs.
This article explores the path forward, offering insights on how to design innovative and effective strategies that leverage human biology and relevant readouts to revolutionize treatments for neurodegenerative disease.
The limitations of ‘one disease–one target–one drug’ dogma to tackle complex diseases
Historically, diseases have been defined only based on their clinical symptoms without any consideration to their underlying pathophysiological mechanisms. Hence, you have probably being developing drugs based on the ‘one disease–one target–one drug’ dogma. While this approach can render positive outcomes for mono-target, monogenic diseases (i.e., selective cyclooxygenase-2 inhibitors for arthritis), for multifactorial ones, such as neurodegenerative disorders, this dogma falls short, as they are usually not caused by a single protein but by signaling networks. 1In fact, most current drugs for such diseases are highly ineffective, highlighting the need for a change of paradigm.
To advance in this direction, the perspective of network medicine is setting the ground for this change. Network medicine intends to redefine disease and its treatment, from descriptive, symptomatic phenotypes to causative molecular mechanisms, also called endotypes. Hence, endotypes are established from all factors (associated risk, driver genes, proteins, and drug targets) that form a de novo disease signaling network. Thus, a disease phenotype or symptom would result from the interactions of various disease networks. 1
Identifying common therapeutic targets for neurodegenerative disorders
As you probably know, the most common treatment approach is multitargeting via combination therapy. However, a simultaneous treatment with multiple drugs is more costly and can cause problems related to different pharmacokinetics, toxicity, and patient compliance. 234 The redefinition of disease according to causal factors instead of symptoms, can help you approach drug discovery with a different perspective.
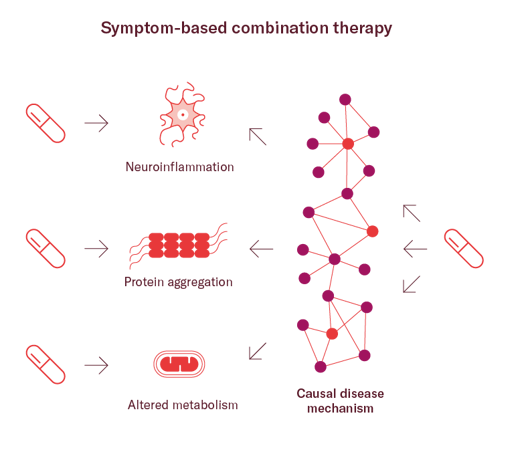
The pharmaceutical industry has recently started to invest on the development of rationally designed multitargeted drugs that could address more than one symptom simultaneously. Such multitargeted drugs may be a better match for complex, polygenic diseases with multiple underlying mechanisms, like neurodegenerative disorders.5
One example you can look at is olanzapine, a multitargeted drug that exhibits nanomolar affinities for over a dozen different receptors. Highly selective anti-psychotic drugs failed to reach the market as they were too selective, but olanzapine succeeded treating resistant schizophrenia.6
Another promising approach you could consider is leveraging shared molecular mechanisms across etiologically different diseases to develop one drug with potential to treat more than one disease.
For example, protein aggregation is a common hallmark shared by multiple neurodegenerative disorders (AD, PD, ALS, FTD, etc.). Therefore, finding a drug capable of eliminating protein aggregates could potentially be effective in more than one disease. In fact, the number of programs aiming to safeguard protein homeostasis or activate protein degradation is increasing. Interestingly, a repurposed multitargeted-drug, rifampin, has shown in vitro and in vivo efficacy to disaggregate toxic oligomers and initial promising results in humans.9
Phenotypic or target-based drug discovery? Getting the best of both
Once you have a mechanistically defined pathway driving a disease, how do you proceed to gain confidence in your findings?
There are at least two main strategies to identify an efficient network approach for the treatment of multifactorial diseases. In the phenotype-based approach, rationally chosen combinations of drugs are tested using cell-based assays.
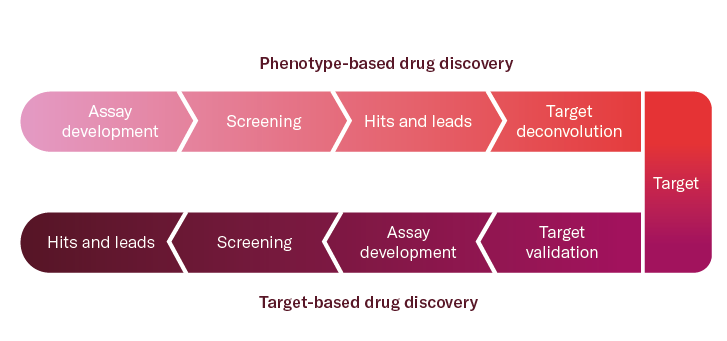
Conversely, the target-based approach starts by identifying crucial genomic, transcriptomic, or proteomic alterations in the network and then searches for drug targets that selectively revert these network changes. Although this approach allows to develop novel, highly effective treatments, target validation is usually complex, long-lasting, and associated with high attrition rates. 8 For this reason, there has been a renaissance of phenotypic drug discovery (PDD) approaches, now focusing on the modulation of a disease phenotype or biomarker rather than a pre-specified target.11
Following a PDD strategy can be particularly advantageous in cases where you don't know the target or/and when the objective is finding a first-in-class drug with a particular mode of action. For example, phenotypic screening can help you identify molecules engaging multiple targets. 5 In contrast, the disadvantage is that you will probably need to go through target deconvolution studies to increase probability of clinical success.
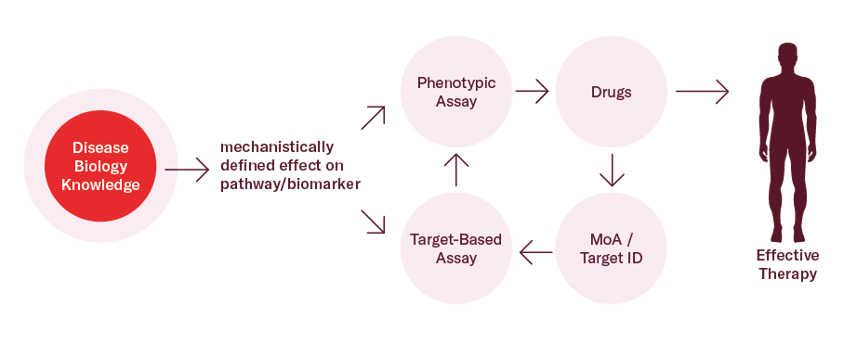
However, the choice is not binary; most often, combinations of the two strategies above are the effective solution you are looking for.
Combining phenotypic screening with target-based drug discovery can provide you with highly relevant information about your compounds and prevent late-stage failures. For instance, for diseases where a pathological target is known, targeted phenotypic screens can be employed from the early stages of discovery to identify the most promising hits and leads based on functional and phenotypic readouts. 5
The impact of choosing the right models for phenotypic screening
A phenotypic assay requires at least two elements: a model system and a readout12,13. Both elements need to have a clear link to disease and replicate, as far as possible, physiologically relevant aspects.
The model
Animal models are not available for some neurodegenerative disorders, and even for diseases for which there are, there is an important lack of translatability. Therefore, advanced, physiologically relevant human in vitro models are urgently needed to increase the efficiency of drug development.
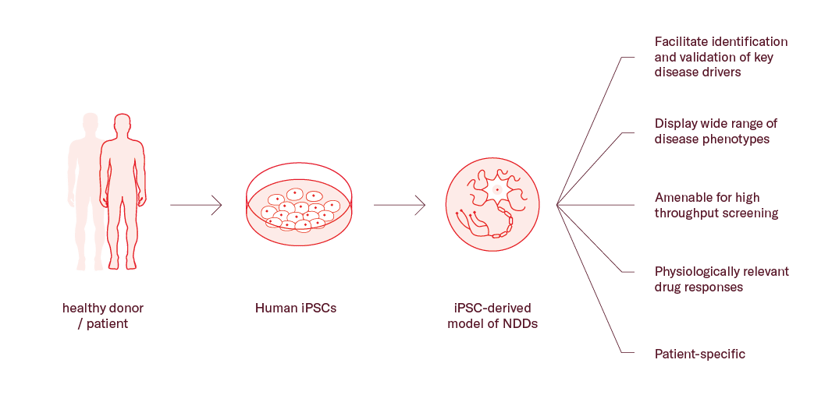
Physiologically relevant assay systems such as those using specific, induced pluripotent cells (iPSCs), are a powerful tool for drug discovery. Importantly, the biggest advantage of such in vitro biological model systems is that they reproduce the molecular mechanism of the disease and can often predict drug efficacy and safety accurately. 3
For instance, CC-90003, an oncological drug tested in a Phase Ia clinical trial was discontinued due to its neuropathic and neurotoxic effects14. Despite having been tested in rodents, these effects were not observed until the drug was tested in humans. Later on, an in vitro phenotypic assay in human derived-iPSCs was able to effectively predict the negative side effects of the drug, demonstrating the power of these models. Therefore, integrating human iPSC in vitro models in your discovery and development programs can reduce the chances of late stage failures.
The readout
The readout should provide information as close as possible to the pathophysiology and clinical end point in patients.12,13 For instance, the combination of an iPSC-based model with a molecular readout, such as endogenous gene expression or protein aggregation, can make more accurate predictions about the potential of drug candidates.
One popular approach to consider is integrating relevant iPSC models with high-content imaging technology. This allows you to study the impact of potential drug candidates on disease-specific biomarkers, cellular dysfunction, and pathophysiological characteristics, which is particularly useful for understanding complex diseases. Moreover, high-content imaging can evaluate multiple parameters in one single experiment, saving time and resources.
When to incorporate human in vitro models into your pipeline?
The answer is simple: at the earliest opportunity. Asking the right questions to the right models is essential to mitigate risks in drug discovery.
With the proper expertise, human iPSC in vitro models can be highly adaptable and augmentable for high-throughput phenotypic research during the hit identification phase of drug discovery.
As you move forward in the discovery funnel, these models can be integrated for hit-to-lead and lead optimization as well. In fact, their complexity can be increased to further mimic physiologically relevant environments. For example, an in vitro triculture system including neurons, astrocytes, and microglia derived from human iPSCs can be used to model cell-cell interactions, neuroinflammation and neurodegeneration linked-phenotypes.
When getting closer to the clinic, the development of 3D culture models and new technologies such as the “organ-on-a-chip,” allow you to analyze the efficacy and safety of drugs at an individual level, in conditions much closer to those observed in vivo.15,16
Conclusions
Neurodegenerative diseases have a complex etiology and often share common disease drivers. The traditional ‘one disease–one target–one drug’ dogma might not be the most appropriate for this kind of disorders and may be partially responsible for the lack of available treatments.
Overall, tackling neurodegenerative diseases requires a change of paradigm, defining diseases by networks and searching for multitargeted treatment approaches.
In this context, including phenotypic readouts and human in vitro models in early drug discovery is critical to promptly unveil the most promising candidates and advance with confidence.
References
- Nogales, C. et al. Network pharmacology: curing causal mechanisms instead of treating symptoms. Trends Pharmacol Sci 43, 136–150 (2022). DOI: 10.1016/j.tips.2021.11.004
- Kellar, D. & Craft, S. Brain insulin resistance in Alzheimer’s disease and related disorders: mechanisms and therapeutic approaches. Lancet Neurol 19, 758–766 (2020). DOI: 10.1016/S1474-4422(20)30231-3
- Wareham, L. K. et al. Solving neurodegeneration: common mechanisms and strategies for new treatments. Molecular Neurodegeneration 2022 17:1 17, 1–29 (2022). DOI: 10.1186/s13024-022-00524-0
- Tan, S. H. et al. Emerging pathways to neurodegeneration: Dissecting the critical molecular mechanisms in Alzheimer’s disease, Parkinson’s disease. Biomedicine & Pharmacotherapy 111, 765–777 (2019). DOI: 10.1016/j.biopha.2018.12.101
- Vincent, F. et al. Phenotypic Drug Discovery: Recent successes, lessons learned and new directions. Nat Rev Drug Discov 21, 899 (2022). DOI: 10.1038/s41573-022-00472-w
- Citrome, L., McEvoy, J. P., Todtenkopf, M. S., McDonnell, D. & Weiden, P. J. A commentary on the efficacy of olanzapine for the treatment of schizophrenia: the past, present, and future. Neuropsychiatr Dis Treat 15, 2559 (2019). DOI: 10.2147/NDT.S209284
- Wermuth, C. G. Multitargeted drugs: The end of the ‘one-target-one-disease’ philosophy? Drug Discov Today 9, 826–827 (2004). DOI: 10.1016/S1359-6446(04)03213-1
- Löscher, W. Single-Target Versus Multi-Target Drugs Versus Combinations of Drugs With Multiple Targets: Preclinical and Clinical Evidence for the Treatment or Prevention of Epilepsy. Front Pharmacol 12, 730257 (2021). DOI: 10.3389/fphar.2021.730257
- Iizuka, T. et al. Preventive Effect of Rifampicin on Alzheimer Disease Needs at Least 450 mg Daily for 1 Year: An FDG-PET Follow-Up Study. Dement Geriatr Cogn Dis Extra 7, 204 (2017). DOI: 10.1159/000477343
- Moffat, J. G., Vincent, F., Lee, J. A., Eder, J. & Prunotto, M. Opportunities and challenges in phenotypic drug discovery: an industry perspective. Nature Reviews Drug Discovery 2017 16:8 16, 531–543 (2017). DOI: 10.1038/nrd.2017.111
- Swinney, D. C. Phenotypic vs. Target-Based Drug Discovery for First-in-Class Medicines. Clin Pharmacol Ther 93, 299–301 (2013).
DOI: 10.1038/clpt.2012.236 - Berg, E. L. The future of phenotypic drug discovery. Cell Chem Biol 28, 424–430 (2021). DOI: 10.1016/j.chembiol.2021.01.010
- Vincent, F. et al. Developing predictive assays: the phenotypic screening ‘rule of 3’. Sci Transl Med 7, (2015). DOI: 10.1126/scitranslmed.aab1201
- Belair, D. G. et al. Investigation Into the Role of ERK in Tyrosine Kinase Inhibitor-Induced Neuropathy. Toxicological Sciences 181, 160–174 (2021). DOI: 10.1093/toxsci/kfab033
- Pandey, S. et al. iPSCs in Neurodegenerative Disorders: A Unique Platform for Clinical Research and Personalized Medicine. J Pers Med 12, 1485 (2022). DOI: 10.3390/jpm12091485
- Lee, G. et al. Large-scale screening using familial dysautonomia induced pluripotent stem cells identifies compounds that rescue IKBKAP expression. Nat Biotechnol 30, 1244–1248 (2012). DOI: 10.1038/nbt.2435